Leverage new funding and flexibility within Medicaid
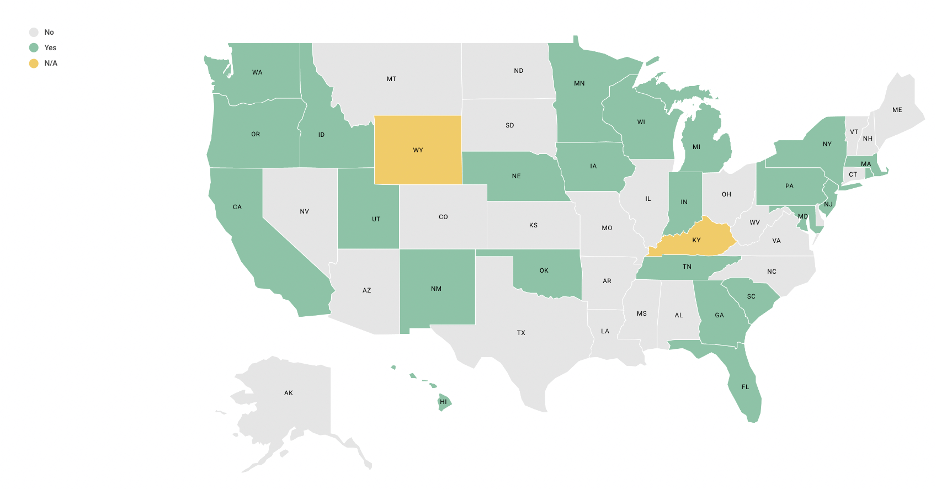
Recent federal funding represents an historic level of investment in HCBS due to the COVID-19 pandemic. Through ARPA, states may draw down an additional 10 percent federal medical assistance percentage (FMAP) for HCBS delivered through March 2022. State plans for spending these additional ARPA dollars provide a window into state priorities moving forward: notably, 30 states propose to use some of this funding to support family caregivers through respite care (12 states), training and education (17 states), and payments to family caregivers (7 states). While this funding is significant, it is short-term and must be spent by the end of calendar year 2024.
State ARPA spending plans represent a significant investment in family caregivers and the care they provide. These plans, which will be updated quarterly, include a range of innovative supports:
- Indiana proposes a caregiver support grant for technology to reduce caregiver loneliness and funding for a gap analysis of family caregiving services.
- Connecticut plans to incorporate supports for caregivers of those with Alzheimer’s disease and related dementias into permanent initiatives. These supports include caregiver assessment, training, respite, care coordination, and the Care of Persons with Dementia in their Environments (COPE) evidence-based support model. The return on investment will be measured via reducing early Medicaid usage, need for paid caregivers, and unpaid caregiver burnout, as well as improving care recipients’ quality of life.
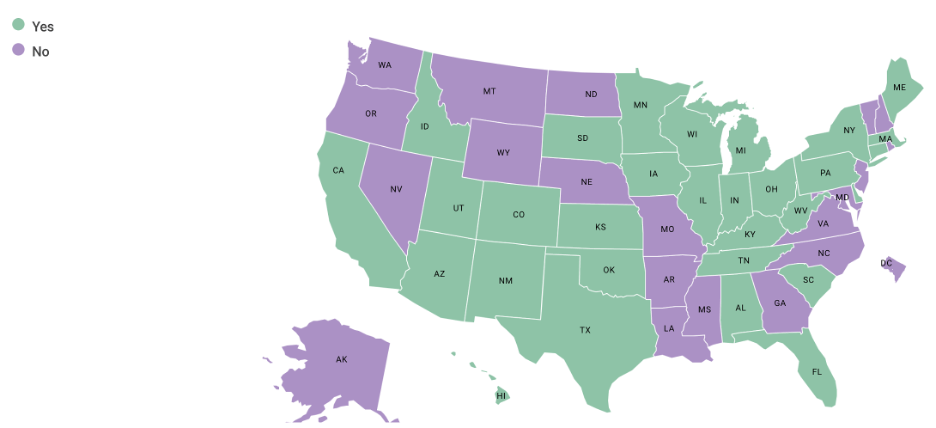
Since the start of the COVID-19 pandemic, CMS has allowed states greater flexibility within state 1915(c) waivers through Appendix K amendments. This policy flexibility resulted in a range of temporary enhancements for Medicaid enrollees and their caregivers during the public health emergency. A NASHP scan of Appendix K amendments found that many states are allowing family caregivers to provide services and receive reimbursement when a hired aide is not available. Six months after the end of the public health emergency, states’ Appendix K amendments are set to end. States will need to assess these flexibilities to determine if they should remain in place for Medicaid beneficiaries and their families.
Reduce overall Medicaid spending and improve care: Washington’s 1115 waiver
Washington’s waiver programs provide additional services to families and are establishing data to better document the return on investment for these programs. The state has successfully reached caregivers of individuals not yet eligible for Medicaid through two programs: Medicaid Alternative Care (MAC) and Tailored Supports for Older Adults (TSOA). MAC supports caregivers of Medicaid-eligible individuals not using Medicaid, and TSOA supports caregivers of individuals not eligible for Medicaid but likely to eventually need Medicaid LTSS. Caregivers of individuals who qualify for these programs are screened using the Tailored Caregiver Assessment and Referral (TCARE) protocol, a tool to assess caregiver needs, and given financial support according to their level of need. Caregivers can spend this money on a wide range of services and supports, including respite, home delivered meals, minor home repairs, training and education, specialized medical equipment, and health maintenance supports, like adult day care and counseling. MAC and TSOA are run under Washington’s Medicaid Transformation project 1115 waiver.
As part of the requirements for its 1115 waiver, Washington has evaluated program cost and quality: a preliminary analysis of key health metrics shows that Medicaid enrollees with families engaged in the program saw a decrease in emergency department visits, hospitalizations, and enrollment in Medicaid HCBS compared to baseline measures. Moreover, surveys conducted with 430 TSOA caregivers and 22 MAC caregivers found high levels of satisfaction with services and a sense of being involved in the support they received.
Washington’s 1115 demonstration waiver was funded by a Delivery System Reform Incentive Payment (DSRIP) initiative which CMS is phasing out. The state is funding a one-year extension (year six) through local intergovernmental transfer funds, which is the plan going forward for a five-year renewal as well.
Support State Rebalancing Efforts
State Medicaid efforts aim for a balance of spending on services in home and community-based settings compared to institutional settings. These rebalancing initiatives are a key focus for states as they navigate current fiscal constraints and envision their future Medicaid service systems. Supporting family caregivers can be an effective rebalancing strategy, as the care they provide allows for a greater number of individuals to remain at home and in the community. Recent research indicates that unmet training needs of caregivers correlated to greater acute care utilization for Medicare home health beneficiaries. Bolstering supports for family caregivers allows for these caregivers to meet the needs of those they serve.
Examples of states that are providing more comprehensive supports to family caregivers through 1915(c) waivers include:
- Georgia’s Structured Family Caregiving program. As part of its 1915(c) Elderly and Disabled Waiver, Georgia provides targeted caregiver supports to unpaid caregivers who live with the Medicaid beneficiary. Services include training, care coordination, and a per diem stipend. Training includes health education, telephonic counseling, and active coordination with care management. The family caregiver receives a minimum of 8 hours of training each year and has the support of other care team members, a health coach, and a registered nurse. Caregivers may qualify for stipends if they are related to the beneficiary biologically and are willing and able to provide care for the beneficiarys assessed needs. Caregivers do not receive stipends for care for a spouse or a minor child.
- Florida’s 1915(b)/1915(c) MLTSS program requires managed care organizations to offer a family caregiver training program as one of several quality enhancements, along with fall prevention in-home and information on end-of-life issues and advanced directives. This program addresses the multilayered financial, emotional, and physical elements of caregiving and outlines the resources available to caregivers in crisis. As described in the waiver, this includes instruction about treatment regiments and other services such as use of equipment specified in the plan of care as well as updates to maintain the care recipient at home. Moreover, Florida managed care organizations are required to establish adequate provider capacity with at least two respite providers serving each rural and urban county of the region.
Address Workforce Shortages through Medicaid Self-Direction
All states use at least one Medicaid self-direction option, which allows beneficiaries to select and pay for direct care aides, including family caregivers, to provide personal care. The extreme shortage of direct care workers is well documented; self-direction can be one strategy for states to both support families and ease workforce shortages in LTSS. State policymakers also note that self-direction can help address disparate access to care in underserved communities, by allowing Medicaid enrollees to choose caregivers from their own cultures and communities or who speak the same language. A NASHP study outlines opportunities and innovations for states to pay family caregivers through their Medicaid self-direction programs.
- California: Extensive use of self-direction as an alternative to out-of-home care. Created in 1974, the In Home Supportive Services (IHSS) program serves over 600,500 low-income older adults and people with disabilities. This Medi-Cal self-direction program allows family caregivers to provide care in the home and receive payment from Medicaid. IHSS is comprised of four programs that each offer special eligibility provisions with a range of personal care, paramedical, and chore services. The first, the IHSS-Residual, provides personal care services for individuals not fully Medi-Cal eligible through a combination of state and county dollars. The second and most utilized program, the Personal Care Services Program, offers services for individuals who are fully Medi-Cal eligible but do not qualify for the Community First Choice Option (CFCO). The third option, the IHSS Plus Option, allows spouses to be eligible providers. The last program, CFCO, is a state plan benefit that provides tailored in-home services and supports for individuals who would otherwise need a nursing facility level of care. This CFCO option also gives states an additional six percent Federal Financial Participation.
- Colorado: Expanding the scope of practice for family caregivers. Colorado’s In-Home Support Services (IHSS) is a participant-directed service delivery option provided in three of its 1915(c) waivers. IHSS is available to both children and adults; parents and other family members are permitted to work as paid attendants. The Medicaid beneficiary or their Authorized Representative may direct their services by hiring, recruiting, training, and scheduling their caregiver (attendant). Attendants are employed by a licensed home care agency that provides 24-hour back-up services, access to a nurse, and Independent Living Core Services. Colorado’s legislature waived the nurse practice act for IHSS; certification and/or licensure is not required for attendants to provide skilled services to the Medicaid beneficiary. The IHSS Agency’s registered nurse provides training and completes skills validation for attendants specific to the beneficiary’s unique health care needs.


