

Lesbian, Gay, Bisexual, Transgender, and Queer (LGBTQ+) Pride Month is currently celebrated in June each year to honor the 1969 Stonewall Uprising in Manhattan, a turning point for LGBTQ+ rights activism in the United States. The LGBTQ+ community is comprised of over 11 million Americans, or 4.5% of the U.S. population with all ages, races, ethnicities, and income levels represented. A history of stigmatization and inequity has led to ongoing health disparities within all LGBTQ+ groups. In fact, 57% of LGBTQ+ people report experiencing discrimination in some part of their life, including 16% in a medical setting. Many delay access to healthcare for fear of discrimination, which can lead
to increased risk of hospitalizations and poor outcomes. Disparities also exist in the physical and mental health of LGBTQ+ individuals, with previous studies showing higher rates of smoking, depression, certain cancers, and physical violence, all of which are risk factors for conditions that can lead to hospitalization. Finally, where a patient receives care can dramatically impact the available resources. Because SHM is represented by hospitalists from across the United States, it is imperative that we understand these regional differences.
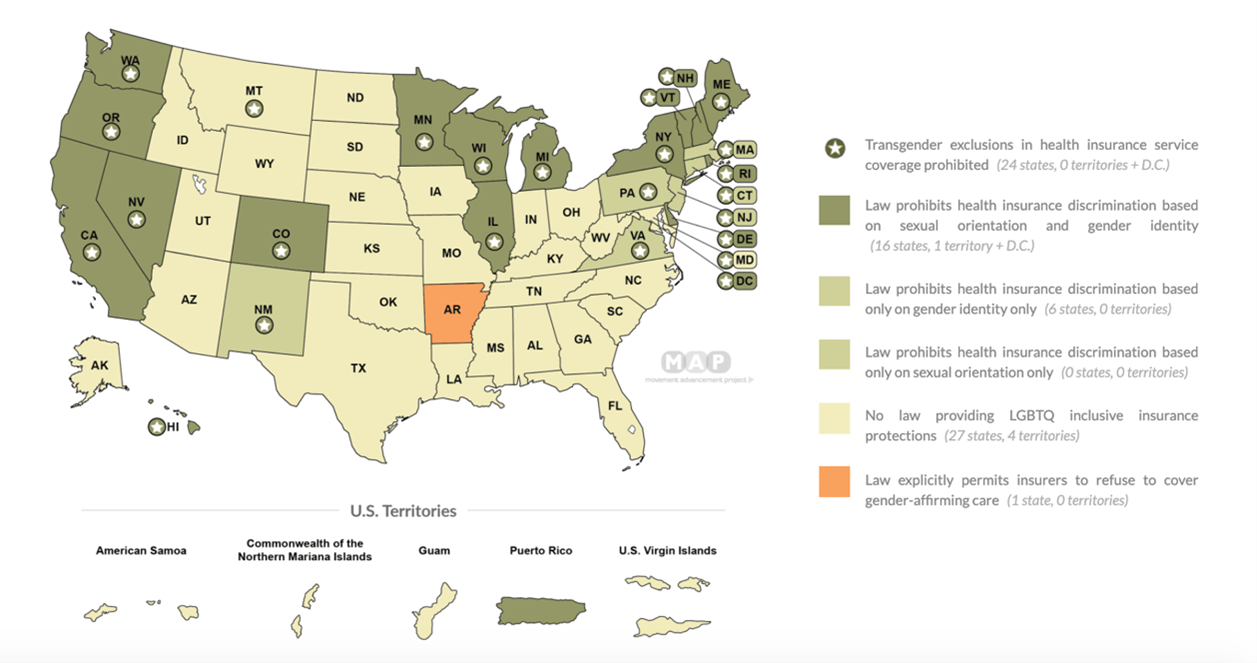
Source: Movement Advancement Project. “Equality Maps: Healthcare Laws and Policies.”
As hospitalists, we are responsible for diagnosis, treatment, and creation of a safe outpatient transition plan, all of which rely on knowing the patient’s social milieu, risk factors, and support systems.
Despite an increasing number of LGBTQ+ individuals, hospitalists often receive little to no formal training in LGBTQ+ health. U.S. and Canadian medical schools average only five hours of LGBTQ+-specific curriculum over four years and highly variable across residency training.
To better understand hospitalists’ experience and clinical comfort in caring for LGBTQ+ individuals, the Society of Hospital Medicine (SHM) Education Committee established an LGBTQ+ Health Task Force which performed a society wide needs assessment to identify gaps in knowledge. Though most hospitalists surveyed had cared for and expressed comfort in interacting with LGBTQ+ patients, there was less consensus about clinical competence. Knowledge gaps included not knowing that bisexual individuals have worse health outcomes when compared to both straight and gay/lesbian peers or recognition of sexual orientation and gender identity as social determinants of health. The systemic discrimination faced by this population can make social aspects of care even more complex. Understanding these barriers and communicating in a culturally responsive, empathic manner is essential to provide equitable inpatient care for LGBTQ+ patients. The gap highlighted in this survey suggests that further education is needed in this area. Not surprisingly, the majority of SHM members who responded welcomed further LGBTQ+ health training.
In addition to delivering content at prior SHM annual conferences and at SHM Converge, the LGBTQ+ Task Force has put together a collection of brief video lectures on the following high-impact areas in LGBTQ+ Health:
- Clinical Documentation (with patients in mind)
- HIV PrEP: inpatient implications and recommendations
- Gender affirming therapy: inpatient implications and recommendations
- How to be an advocate at the population/policy level
- LGBTQ+ = social determinant, even for hospitalists
It our hope with these brief, 10-15-minute quick lectures, providers will learn practical tips and tricks to provide more equitable care and become allies for their LGBTQ+ patients.
This material has been released in conjunction with LGBTQ+ Pride Month. With a growing and aging LGBTQ+ population, improving providers’ clinical knowledge and cultural humility is essential to the provision of more equitable care for this underserved population.
Click here to access the content.
Leave A Comment