Efforts to make health care more affordable can target several problems that lead to high and rising hospital costs. Hospital and physician costs make up the majority of medical expenditures in the U.S. and rising hospital prices directly contribute to higher insurance premiums and make care less affordable for consumers. As seen below, identifying the right policy tool requires first identifying which “cost driver” should be addressed – this could be the lack of transparency in costs and pricing or the unchecked growth in hospital prices. As these issues are interwoven, these different policy tools complement one another and can be used together to combat the many contributors to high costs.
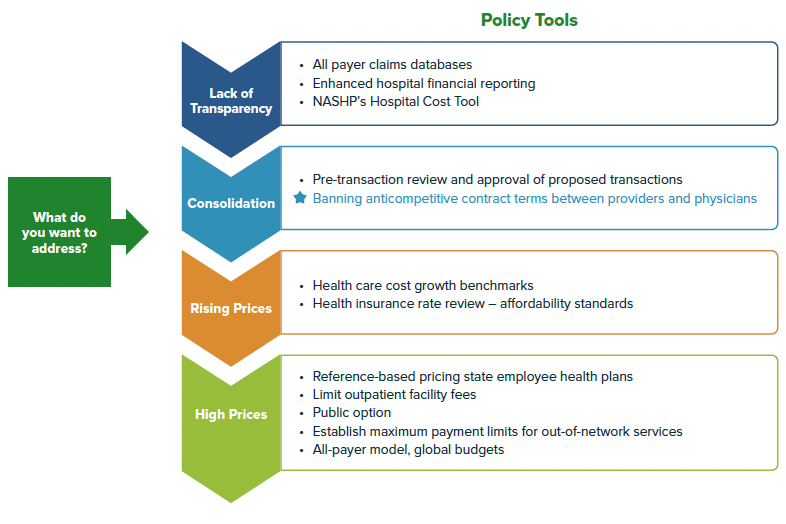
One of these contributors, hospital consolidation, has played an outsized role in making health care less affordable for consumers and employers. Evidence suggests that consolidation leads to higher hospital and provider prices and higher total expenditures – all while having little to no impact on improving quality of care for patients, reducing utilization, or improving efficiency. In many states, hospital markets are already consolidated so it’s not enough to try to prevent consolidation from occurring through pre-transaction review. The National Academy for State Health Policy (NASHP)’s Model Act to Address Anticompetitive Terms in Health Insurance Contracts is one policy tool to target the negative impacts of consolidation and give states authority to limit already dominant health systems from abusing their market power. Essentially, by prohibiting anticompetitive contracting, a state will be helping payers, including employers on behalf of their employees, navigate a consolidated health system to achieve lower costs without affecting access to care.
Prohibiting anticompetitive contract terms will help level the playing field for negotiations between insurers and large health systems, allowing insurers to negotiate lower in-network prices and design networks with the highest quality, lowest cost providers. Without these prohibitions in place, health systems may leverage their “must-have” providers to restrict insurers’ ability to design high-value provider networks.
Due to existing requirements on insurers known as network adequacy, certain providers may be deemed a “must-have” or a facility or doctor that must be in-network for a health plan to meet existing requirements. Some providers may also be considered “must-haves” because of the providers’ reputation to entice employers and consumers to enroll their plans, an insurer must include those providers in-network. Knowing this, large consolidated systems can “tie” certain providers to “must-have” facilities, essentially demanding an insurer include other, often more expensive providers in-network. In some cases, health systems may demand all of their providers are in-network (all-or-nothing) or are included in the most preferred tiers (anti-tiering), meaning they are very accessible even if they are expensive. These various anticompetitive contracting terms mean that insurers and third-party administrators, often working on behalf of self-funded employers, are limited in their ability to negotiate lower prices or to develop innovative programs to improve quality or access.
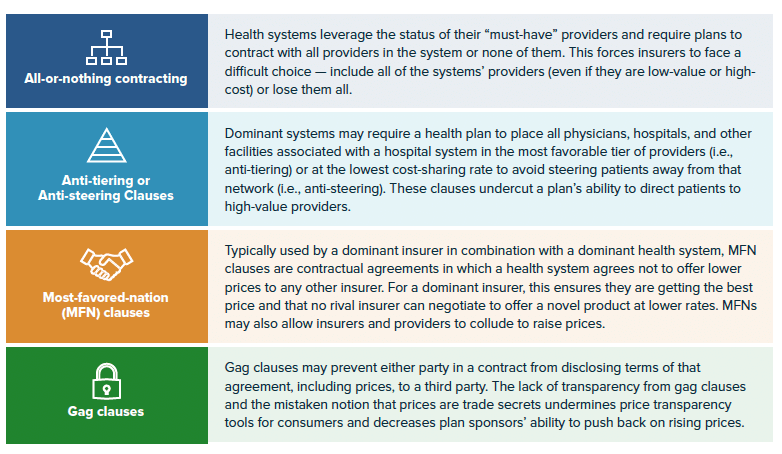
NASHP’s model bill prohibits four types of anticompetitive contracting terms: all-or-nothing contracting, anti-tiering or anti-steering clauses, most favored-nations (MFN) clauses, and gag clauses. The chart below details how each contract clause may be used. The model also gives a state’s insurance commissioner or attorney general the ability to add other clauses through regulation that may result in anticompetitive effects. This flexibility is important as dominant health care entities’ contracting strategies may evolve to protect their market share and raise prices in response to these prohibitions.
As of June 2022, several states have introduced NASHP’s model, and several others had already prohibited some of these anticompetitive contracting terms. In 2021, Nevada enacted a law to prohibit all-or-nothing contracting, joining Massachusetts which has prohibited these clauses in limited or tiered-network plans for more than a decade. Nevada and Massachusetts also restrict the use of anti-tiering or anti-steering clauses. Seven states have banned gag clauses and 19 states have restricted the use of most-favored-nation clauses, although the language varies by state.


