Behavioral health crisis care consists of a range of interventions for people at risk for acute behavioral health issues, experiencing crisis, and engaged in recovery.
Federal guidelines for behavioral health crisis care provide specific guidance on core elements of care and considerations for the unique implementation challenges in rural and frontier areas. As state policymakers advance rural behavioral health crisis care, they are employing innovative approaches to overcome challenges of distance, limited resources, cultural differences, and workforce shortages.

The State Perspective on Rural Behavioral Health Crisis Services
This brief presents considerations and emerging state strategies for bolstering the rural behavioral health crisis care continuum at each level of care as defined by the Substance Abuse and Mental Health Services Administration. Some examples are drawn from advances in states that participated in NASHP’s Policy Academy on Rural Mental Health Crisis Services. Get additional information on this policy academy.
Early Stages of Crisis
In rural areas, intervening early to address behavioral health crises can be especially challenging due to increased social isolation, stigma (including self-stigma), and less access to a full continuum of care and resources. Where behavioral health resources that are tailored to meet the unique needs of local communities exist, they are often scattered and difficult to scale.
Examples such as Alaska’s Behavioral Health Aide (BHA) program and Wyoming’s statewide expansion of Mental Health First Aid offer strategies to address workforce shortages, increase health literacy, and bring culturally-informed approaches to underserved communities. Collectively, these approaches build capacity for intervening in early stages of crisis for people living in rural and frontier areas.
In Alaska, BHAs are a non-licensed provider type employed within the Alaska Tribal Health System, serving rural and remote communities populated mostly by Alaska Natives. They are certified by the Community Health Aide Program Certification Board and supervised by master or doctoral level clinicians. BHAs provide a wide range of culturally relevant, community-based mental health and wellness services, and connect people to higher levels of care when needed.
In Wyoming, the state legislature appropriated American Rescue Plan Act funding to the state’s Department of Health to expand Youth Mental Health First Aid training to:
- Two trainers in each county
- One trainer in each school district
- One trainer in each community college district
- One trainer in the University of Wyoming
Youth Mental Health First Aid is an evidence-based course that trains participants to identify and understand serious behavioral health issues in young people. Youth Mental Health First Aid instructors help youth in crisis receive professional help, when needed, and host instructor training courses for communities that work with youth on an ongoing basis.
Call Centers
Launched in July 2022, the 988 Suicide & Crisis Lifeline presents a unique opportunity for rural areas. Since most crisis calls are resolved by phone, the 988 Lifeline and related behavioral health crisis hotlines serve as crisis interventions in and of themselves. Having such an accessible intervention (which includes phone, text, and chat options) is especially important in rural areas where mobile team response times may vary.
An example of a state call center that has managed high demand from rural areas is the Georgia Crisis and Access Line (GCAL). Operated by Behavioral Health Link, GCAL is available 24/7, 365 days a year and is accessible by calling an existing hotline number (1-800-715-4225). Those with Georgia area codes who call 988 are usually routed to GCAL. (Georgia state officials recommend that people in crisis call GCAL over 988 until at least July 2023 because GCAL routes directly to in-state providers, while 988 may route to a national hub not in the state.) The professionals at GCAL provide crisis intervention services by phone and, if needed, dispatch mobile crisis teams and link individuals to urgent services.
In addition to being able to call GCAL, Georgians can download the My GCAL app to access GCAL via text and chat 24/7 — a development that is particularly beneficial for youth. The state employs a strong data-driven approach, tracking and sharing data with the public regularly.
In Arizona, the Arizona Health Care Cost Containment System (AHCCCS), provides Medicaid reimbursement for crisis services statewide via AHCCCS Complete Care Contractors with Regional Behavioral Health Agreements (ACC-RBHAs). Services are available to all Arizona residents regardless of health insurance coverage.
To operate the state’s 24/7 crisis hotline (1-844-534-HOPE), the ACC-RBHAs selected Solari Crisis & Human Services along with La Frontera Empact. Those who call 988 with an Arizona area code are routed to the statewide call vendor responsible for operating the ACC-RBHA crisis lines and can be easily transitioned into the local crisis system of care if a mobile team or facility-based service is needed for additional support.
Along with the ACC-RBHAs, AHCCCS has established intergovernmental agreements (IGAs) with tribal nations to provide them with funding for behavioral health crisis services via Tribal Regional Behavioral Health Authorities (TRBHAs) based on the needs and requests of each individual tribe. Arizona tribes, regardless of having an established an IGA directly with AHCCCS, are also able to connect with the ACC-RBHA serving their region for behavioral health crisis services as needed.

Source: AHCCCS
Mobile Crisis Teams
In rural areas, mobile crisis teams’ responses to behavioral health crisis calls can be slowed due to long travel distances and limited staffing. Some states have creatively addressed these challenges.
In South Dakota (a participating state in NASHP’s Policy Academy on rural behavioral health crisis), the Virtual Crisis Care program provides law enforcement with 24/7 access to behavioral health professionals who can assist in responding to people experiencing a mental health crisis. It also ensures that those working in the criminal justice system have access to the resources they need to help people with mental illness, regardless of where they live. This service offers de-escalation, stabilization, safety assessments, and connections to local behavioral health resources for follow-up care.
Arizona’s mobile crisis teams respond to a call in an average of 30–40 minutes anywhere in the state, including in rural areas. To achieve this, Arizona’s mobile crisis teams are enabled with live GPS tracking and coordination so that the nearest available mobile crisis team is dispatched to a person in crisis across city and county lines.
In addition to being GPS enabled, mobile crisis teams in Arizona are often co-located in 911 centers, police departments, jails, and tribal health centers in areas that face a higher volume of crisis calls. These co-locations in areas with higher crisis utilization rates allow mobile crisis teams to respond in a timely manner. For example, in Mohave County (the fifth largest county in the contiguous United States), there are two co-locations at police departments that have yielded an average response time of 25 minutes from October 2022 to December 2022.
Arizona uses a braided funding approach, including Medicaid reimbursement, state appropriated funds, and federal grants to provide a “firehouse model.” This means teams are available for blocked periods of time during peak, off peak, and on call hours — ensuring that, despite volume fluctuations, there is always a team available.
In addition, this funding model ensures a response in which care is provided for all mental health emergencies regardless of a person’s health coverage status (e.g., Medicaid, private insurance, no insurance) consistent with a true “no wrong door” model.
Crisis Stabilization/Receiving Facilities
- Adjusted administrative rule with adapted minimum standards and expectations (such as staffing requirements)
- Adjusted Medicaid reimbursement rates for rural adaptations
- Coordinating and subcontracting with urban psychiatric providers via telehealth in rural settings
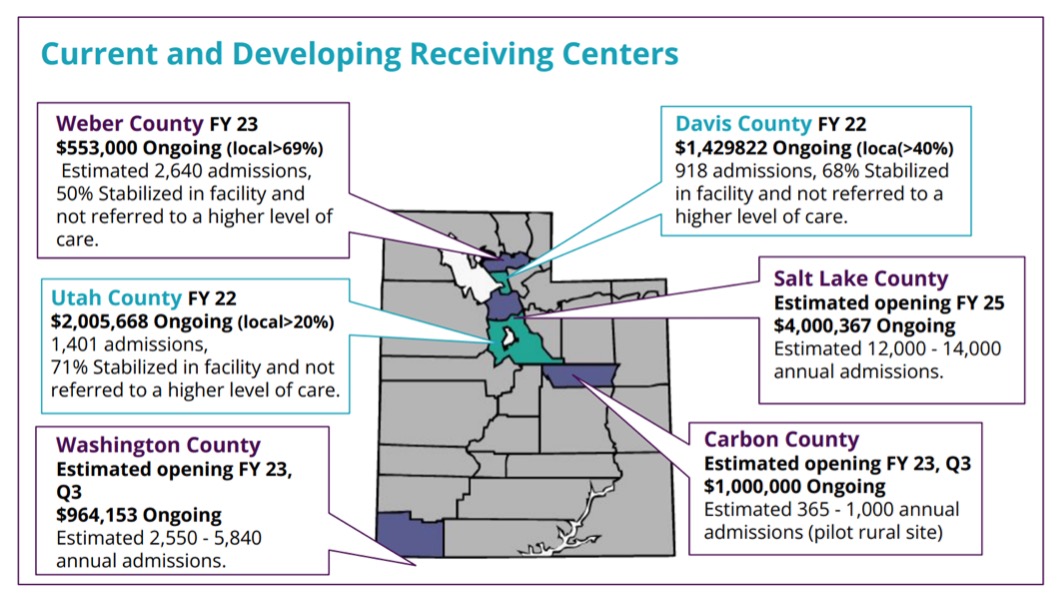
Source: Nichole Cunha, UT
- Telephone and telehealth-based responses (in partnership with 988)
- Statewide mobile crisis teams for both children and adults
- Psychiatric urgent recovery centers
- Crisis centers
- Psychiatric hospitals
Post-Crisis Support
Coordinating connection to ongoing care to avoid or support recovery after a behavioral health crisis is an essential component of crisis care. However, in rural areas, it can be especially challenging for individuals to be linked with regular post-crisis support.
Tennessee’s Project Rural Recovery offers a potential strategy for delivering post-crisis support in resource-limited rural areas. Since March 2020, Tennessee has leveraged a five-year federal grant to provide free, integrated behavioral and physical health services to 10 rural counties in the state.
Currently, Project Rural Recovery consists of two mobile health clinics that offer mental health counseling, behavioral health screenings, and outpatient substance abuse services along with primary health care. These mobile clinics are available once a week in each of the 10 rural counties served. Due to the success of the program, state policymakers have awarded $6.3 million of American Rescue Plan Act funding to add two mobile health units and double the number of counties served starting in spring 2023.
Acknowledgements
This work was supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) as part of a financial assistance award under the National Organizations of State and Local Officials (NOSLO) cooperative agreement totaling $836,859.00. The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement, by HRSA, HHS, or the U.S. Government. For more information, please visit HRSA.gov. NASHP thanks the many state officials from Alaska, Arizona, Georgia, Oklahoma, South Dakota, Tennessee, and Wyoming who contributed to this resource by sharing detailed information about efforts in their states to advance best practices in addressing behavioral health crisis in rural areas.
