Mary Madison, RN, RAC-CT, CDP
Clinical Consultant – Briggs Healthcare
This research letter was published in the JAMA Health Forum on February 25, 2022.
“The COVID-19 pandemic has disrupted the US health care workforce owing to changes in the use and finances of health care clinician offices and institutions, increased health risks, burnout from increased patient burdens, and child care disruptions.1–4 While federal programs have provided financial assistance to hospitals and institutions,1 the net effect of these forces on health care employment levels and wages has not been examined. Understanding trends in employment levels by health care settings and locations is critical for planning and responding to public health crises.
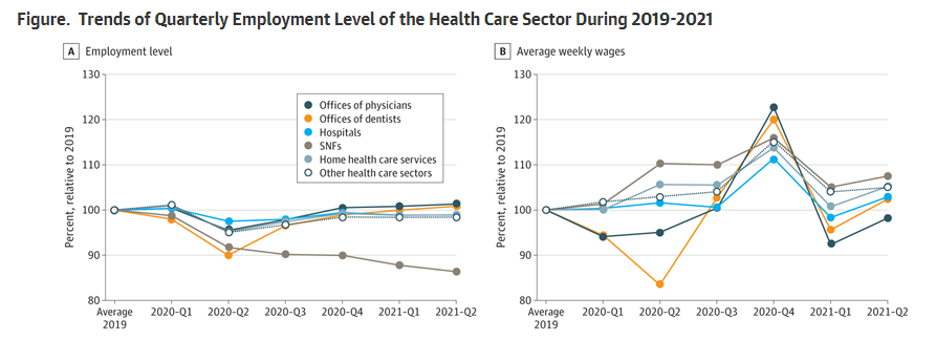
Health care employment levels declined suddenly, from 22.2 million in 2019 to 21.1 million, in 2020-Q2—a 5.2% decline (vs a 9.0% decline in all industries), and considerably rebounded to 21.8 million in 2021-Q2. Average wages within the health care sector increased at a lower rate relative to all industries’ changes (2020: 5.0% vs 6.7%; and 2021-Q2: 1.5% vs 6.9%).
Employment declines varied by types of health care organizations (Figure), with the largest declines in 2020-Q2 among offices of dentists (10.0%) and SNFs (8.4%). The smallest declines were among hospitals (2.5%) and offices of physicians (4.6%). While the employment level of most health care sectors rebounded to the pre-COVID levels in 2021-Q2, there were more declines in employment among SNFs (13.6% decline compared with 2019). Employees in SNFs exhibited the largest wage increases in 2020 (9.5%) and 2021 (6.3%), compared with 2019.
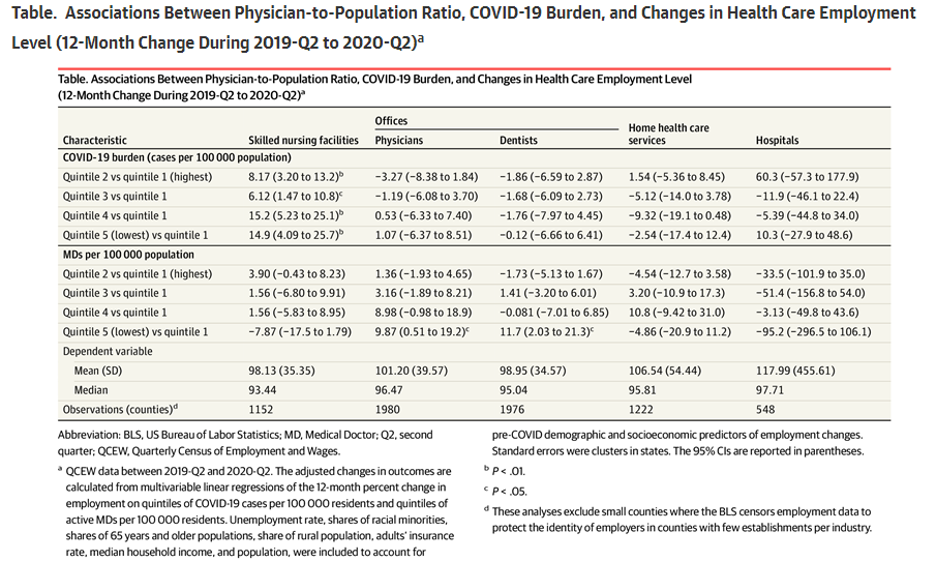
The Table highlights a statistically significant and positive association between the COVID-19 burden and 12-month percent change in employment levels among SNFs: the adjusted 2020 employment level in SNFs relative to 2019 was 105.2% among counties with the lowest quintile of COVID-19 cases and only 90.4% among counties with the top 20% burden (P = .008). Compared with the top 20%, counties with the lowest physician-to-population ratios tended to have higher adjusted employment levels in offices of physicians (107.8% vs 97.9%, P = .04) and among offices of dentists (110.1% vs 98.4%, P = .02). These associations were not statistically significant among other types of institutions.
Protecting the health care sector has been a priority in the pandemic.6 We documented changes in health care employment levels and wages during 2020 and 2021. We found substantial employment declines among SNFs, which were more severe in counties with high COVID-19 burden. The 2020 declines in employment among offices of physicians and offices of dentists were relatively smaller in counties with lower pre-pandemic physician-to-population ratios.
Limitations include the exclusion of certain counties with censored data and our inability to examine mechanisms for workforce changes. Future research is needed to understand if organizations are demanding fewer workers or fewer workers are willing to work at health care positions. Overall, our results imply that intensified early efforts are needed to protect the health care workforce in future pandemics.”
You can download the PDF version of this open access article via the hyperlink in the first paragraph of this blog (you’ll see the Download PDF in the upper left as well as to the right on that landing page).
