This toolkit is a resource for state policymakers interested in strategies to address high and rising hospital and health system costs. The toolkit includes resources to better understand the hospital cost data, model legislation and resources that the National Academy for State Health Policy (NASHP) developed with guidance from states officials, as well as data and legal experts. For additional information, email Maureen Hensley-Quinn.
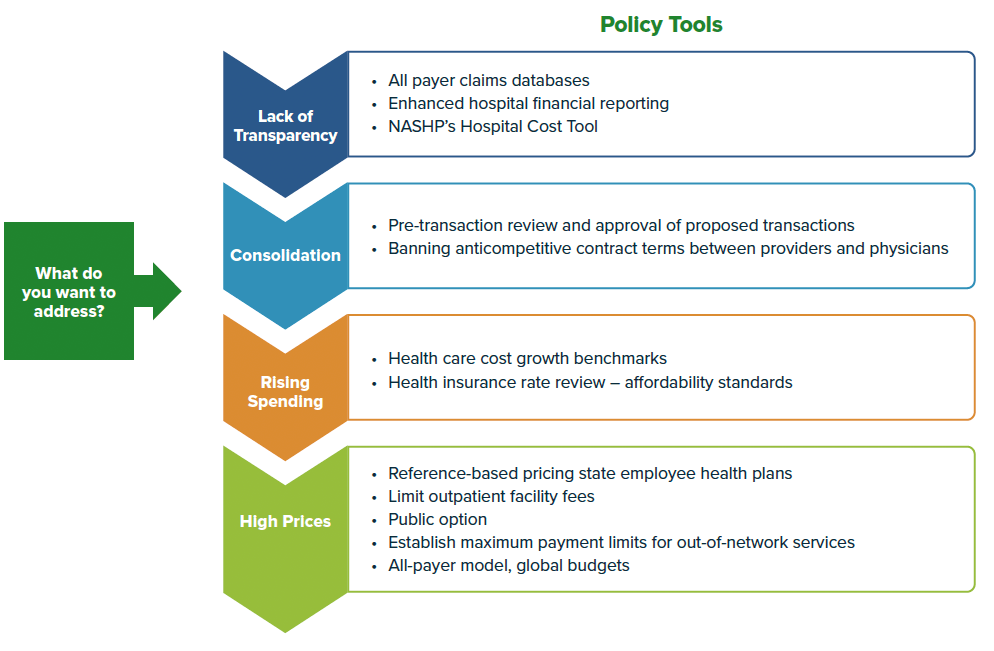
To help state policymakers and their partners understand hospital costs from profits and losses on different payers to how much a hospital needs from commercial health plans to cover their expenses (also known as a hospital’s breakeven point), NASHP created the Hospital Cost Tool. Using annual hospital Medicare Cost Reports, the tool highlights a variety of different metrics for almost 5,000 hospitals.
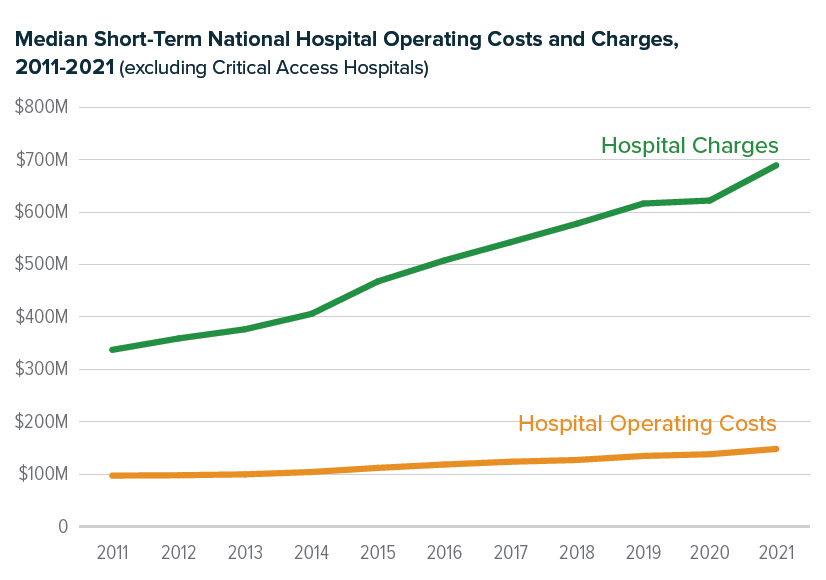
See data below from NASHP’s Hospital Cost Tool Median national hospital charges vs. operating costs
Resources
- Hospital Cost Tool, which includes visual dashboards of multiple metrics, as well as a downloadable spreadsheet of all of the data within the website and more.
- NASHP Explainer: What is Breakeven?
- Q&A: What can states learn from the hospital cost tool?